

Campaigns, Policy Updates
The National Women’s Health Network’s 2024 Policy Agenda
January 24, 2024
---
Consumer Health Info
Publication Date: June 18, 2019
By: NWHN Staff

Opioid dependency is a bodily adaptation that is likely to disproportionately affect women, because they are more likely to develop opioid dependency in a shorter period of time, compared to men.
America is in the midst of an epidemic of opioid use disorder and addiction – in 2017, there were 70,237 drug overdose deaths, two-thirds of which involved opioids. Overdose deaths have increased almost 6 times since 1999, and accidental drug overdose is now the leading cause of death in the U.S. among those under age 50 (the highest overdose rates are among those aged 25-44). An estimated 130 Americans die from overdose every day. For more information about the history and health implications of the opioid epidemic, see the NWHN’s Consumer Health Info on this topic.
Women may also be more vulnerable to cravings and relapses that are indicative of addiction. For example, while men and women are prescribed similar amounts of opioids for pain after common procedures such as colectomy, rotator cuff surgery, and knee replacement surgery, 40% more women were still taking opioids 90 or more days post-surgery, an indication of possible opioid addiction or dependence.
This problem is exacerbated by the fact that women receive two-thirds (65%) of all U.S. opioid prescriptions. Moreover, prescriptions given to women are often for higher doses, and for a longer period of time, compared to prescriptions provided to men. The results are devastating: women’s mortality rates from opioid overdose increased 507% between 1999 and 2016, compared to an increase of 321% for men.
Tragically, the nation has been largely unresponsive to women’s distinct risks and needs when it comes to opioid use disorder. According to a 2015 national survey, less than half (44%) of treatment programs provided special programs and/or groups tailored to women’s needs, and only 21% offered programs or groups for pregnant or postpartum women.
Women’s risk of opioid dependency and opioid use disorder demand a variety of interventions. Here’s what the NWHN recommends in order to continue making progress to advance women’s health.
 Expanding Medicaid to cover more low- and moderate-income people is essential to protecting women’s health. The Affordable Care Act (ACA) authorized states to expand their Medicaid eligibility levels and cover significantly more uninsured Americans. Assessments of Medicaid expansion’s impact are showing that people are more likely to access care earlier, less likely to have catastrophic medical expenses, and more likely to self-report being in “excellent” health.
Expanding Medicaid to cover more low- and moderate-income people is essential to protecting women’s health. The Affordable Care Act (ACA) authorized states to expand their Medicaid eligibility levels and cover significantly more uninsured Americans. Assessments of Medicaid expansion’s impact are showing that people are more likely to access care earlier, less likely to have catastrophic medical expenses, and more likely to self-report being in “excellent” health.
With respect to the opioid epidemic, Medicaid expansion is associated with increased use of effective treatments of opioid use disorder as well as better coverage of treatment for pregnant women seeking treatment for addiction. For women who can’t get Medicaid because they live in non-expansion states, or who fall into the coverage gap, screening and treatment for opioid use disorder is frequently inaccessible.
Women-particularly single mothers and women of color-are more likely to be poor compared to men, they are also more likely to lack health insurance, and suffer poor health as a result. For this reason, the NWHN has long supported Medicaid expansion as a critical factor in promoting women’s health. Yet, despite the clear public health benefits, 14 states have chosen not to expand their Medicaid programs to date.
Unfortunately, even in expansion states, access to opioid treatment may be challenging. Nine state Medicaid programs do not cover methadone; 14 states do not cover the buprenorphine implant; and 18 states do not cover extended-release buprenorphine-all of which are effective Medication-Assisted Treatments (MAT) for opioid addiction. And, although MAT programs help people cope with cravings and withdrawal symptoms, some states specifically do not reimburse providers for MAT’s use to treat addiction, limiting access to life-saving care.
Having coverage and access to effective treatment interventions are essential to combating the opioid epidemic. For this reason, the NWHN advocates for Medicaid expansion in all states, and reimbursement for all forms of effective interventions for opioid addiction and dependency.
 The Food and Drug Administration (FDA) doesn’t have the best track record when it comes to opioid oversight. In 2001, the FDA expanded the approved use of Oxycontin from short-term use to “daily, around-the-clock, long-term… treatment.” Later, in 2016, the FDA could have intervened or spoken out against doctors who were incorrectly prescribing overly powerful opioids to patients with low tolerances-but the agency did nothing. Since then, the FDA has tried to take a more active role in addressing the opioid crisis, within the limits of its jurisdiction. The NWHN applauds the FDA’s explicit support of new effectiveness measures for MAT clinical trials that involve assessing products against “patient-reported experiences” rather than just clinical outcomes. The development of new treatment options in this realm has the potential to make meaningful differences for women who struggle with addiction.
The Food and Drug Administration (FDA) doesn’t have the best track record when it comes to opioid oversight. In 2001, the FDA expanded the approved use of Oxycontin from short-term use to “daily, around-the-clock, long-term… treatment.” Later, in 2016, the FDA could have intervened or spoken out against doctors who were incorrectly prescribing overly powerful opioids to patients with low tolerances-but the agency did nothing. Since then, the FDA has tried to take a more active role in addressing the opioid crisis, within the limits of its jurisdiction. The NWHN applauds the FDA’s explicit support of new effectiveness measures for MAT clinical trials that involve assessing products against “patient-reported experiences” rather than just clinical outcomes. The development of new treatment options in this realm has the potential to make meaningful differences for women who struggle with addiction.
The NWHN supports these efforts-but thinks the agency can go further.
First, the FDA has sent warning letters to companies that sell opioids illegally online. Yet, the FDA has stopped short of imposing criminal penalties for most groups through its Office of Criminal Investigations (OCI). It may be time for higher criminal and/or financial penalties to further discourage these activities.
Second, the FDA is showing that it learned from a prior mistake with respect to “abuse-deterrent” (AD) opioid formulations. AD formulations are used to make opioids less effective when they are crushed (so they can be snorted) or dissolved (so they can be injected). Oxycodone is one of many opioid drugs with new, abuse-deterrent technology designed to limit its misuse. As a result of this technology, oxycodone’s abuse by these methods decreased 48% in the 3 years after the introduction of the AD formulation- but oral misuse increased by 49%. Additionally, studies have found an increase in the abuse of either other prescription opioids (like morphine) or heroin, suggesting that people simply switch to abusing a different drug. According to the Centers for Disease Control and Prevention (CDC), oxycodone remains among the top three drugs involved in prescription opioid overdose deaths, despite these AD reformulations.
After approving a supposedly AD reformulation of a different opioid, oxymorphone hydrochloride, in 2011, nasal abuse rates of the drug dropped, but rates of intravenous abuse increased. The drug was ultimately pulled from the market in 2017. In 2018, a different company sought approval of a somewhat similar reformulated version of oxycodone hydrochloride but-in a rare move-the FDA did not approve the drug.
The NWHN applauds the FDA for not making the same mistake twice, but we believe the agency should be more vocal about the limitations of AD formulations in general. “Abuse-deterrent” is not the same thing as “less addictive.” While the FDA’s promotion on these new formulations may lead to fewer new opioid addictions, they don’t necessarily help people who are currently struggling with addiction-as noted, people may simply switch to more accessible illicit drugs in response to the AD reformulation measures.
Third, the NWHN wants to see the FDA do a better job around the new opioid use disorder products on the market. The agency has incentivized manufacturers to create diagnostic or therapeutic products to address addiction and opioid abuse, or to offer pain mitigation-as a result, several new products have been rushed to market through the FDA’s Innovation Challenge (IC). While the epidemic calls for a rapid response, we believe this must include effective measures to protect consumer safety. We call on the FDA to create discrete and enforceable timelines for IC products’ post-market studies and formal applications so they can conduct normal reviews. This is essential for both providers and patients to receive real-world safety and efficacy information for informed decision-making. Such studies should include patient-reported endpoints about a drug’s effectiveness in addressing the cravings and impulses that characterize addiction.
 Substance use during pregnancy has been linked to serious, negative health outcomes during pregnancy, childbirth, and the post-partum period. Starting in January 2020, the Centers for Medicare and Medicaid Services (CMS) will fund a new program, the Maternal Opioid Misuse (MOM) model, to improve care coordination for pregnant and postpartum Medicaid beneficiaries experiencing opioid use disorder. The program, which will operate in up to 12 states, will provide access to critical essential physical and behavioral health services (including MAT), as well as “maternity care, relevant primary care services, and other mental and behavioral health services beyond MAT.” The NWHN applauds this response to the opioid epidemic, which is far more likely to be effective than the punitive approaches adopted by too many states.
Substance use during pregnancy has been linked to serious, negative health outcomes during pregnancy, childbirth, and the post-partum period. Starting in January 2020, the Centers for Medicare and Medicaid Services (CMS) will fund a new program, the Maternal Opioid Misuse (MOM) model, to improve care coordination for pregnant and postpartum Medicaid beneficiaries experiencing opioid use disorder. The program, which will operate in up to 12 states, will provide access to critical essential physical and behavioral health services (including MAT), as well as “maternity care, relevant primary care services, and other mental and behavioral health services beyond MAT.” The NWHN applauds this response to the opioid epidemic, which is far more likely to be effective than the punitive approaches adopted by too many states.
Addiction and substance use has led to the arrests and incarceration of pregnant women across the country on charges of abuse, neglect, and reckless endangerment of the fetus. In 23 states and the District of Columbia, substance use during pregnancy is considered to be child abuse in civil child-welfare statutes; in 3 states it is grounds for detaining a woman in an institution. These laws are disproportionately enforced against women of color and low-income women. For example, Amnesty International reports that in Tennessee, one-quarter of the state’s arrests for prenatal substance use occurred in Shelby County-a majority Black county-even though Shelby has one of the state’s lowest rates of babies exposed to opioid drugs prenatally. In states like these, pregnant people who are struggling with opioid use disorder avoid seeking addiction treatment and other forms of medical care-including prenatal and postnatal care-due to reasonable fears that they may be arrested, incarcerated, and/or lose custody of their children.
Women need clear, accessible information about their medical options and freedom from police involvement in their medical decisions. State lawmakers should modernize their laws so that pregnant people do not risk arrest or prosecution when they are struggling with addiction. States should promote access to maternal health care, evidence-based treatment services, and the full range of sexual and reproductive health care services. States should also explicitly guarantee that pregnant people will not be tested for drugs without their knowledge and explicit consent.

One important step in addressing the opioid epidemic is to encourage the use of non-opioid pain treatments. As the NWHN has written, except for end-of-life care, opioids should not generally be used for chronic pain. Not only are they dangerous and addictive, but opioids also actually increase pain over time-by increasing sensitivity to pain, they worsen the problem they are supposed to solve. Yet, 9 out of every 10 patients who have surgery are prescribed opioids for pain management and receive too many pills-an average of 85 pills each. It’s estimated that this practice results in 3.3 billion unused prescription opioids becoming available for non-intended use.
Our view aligns with evidence-based guidelines from the federal Department of Health and Human Services, including the CDC, which prioritize non-opioid pain management techniques as first-line pain treatments. A recent study indicates that reducing the number of opioid prescriptions for acute pain, partnered with reformulation and proper disposal, can help reduce the number of opioid-related deaths over a 10-year span.
Advancing this goal will take the engagement of third-party insurance insurers to incentivize health providers actions by broadening and standardizing reimbursement policies for pain management. A recent study found that insurers might cover a 30-day opioid prescription for pain management and, simultaneously, restrict the number of physical therapy visits for the same purpose. Health care insurers should offer more comparable coverage for non-drug and non-opioid therapies so both patients and providers can consider them realistic and affordable options for pain management, and exhaust those options before an opioid prescription is given to a patient. These alternative therapies may include physical therapy, acupuncture, counseling, and/or over-the-counter (OTC) medications. Insurers can also take steps to reduce the risk of long-term addiction and dependence by limiting the number of days an opioid prescription is covered for new patients.
Together these policy changes have the potential to increase women’s access to non-addictive, non-pharmaceutical pain relief treatments and reduce the risk of new opioid addictions.
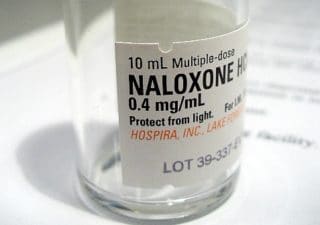
Naloxone is a drug that can help reverse an overdose by enabling unconscious overdose victims to breathe again. It has no potential for abuse and has been safely used for decades. Between 1996 and 2014, the administration of naloxone helped rescue almost 27,000 individuals from overdose deaths. Yet, not everyone gets equal access to this life-saving drug. One study found that first responders were three times more likely to administer naloxone to men than to women when responding to a patient who had overdosed. The NWHN believes that all first-responders should be required to administer naloxone on an equal basis to anyone experiencing an overdose.
Many communities have created programs and policies to ensure that naloxone is widely available for use in the community-not just by first responders. Nationwide, state regulators can do more, however, to ensure that the product is readily available when needed. by allowing and/or promoting community-level prescriptions, co-prescriptions, third-party prescriptions, and prescribing power for pharmacists. Other ideas include making naloxone OTC and placing naloxone kits in the AED cabinets that are found in many in public spaces, like airports.

The U.S. does not have enough substance abuse prevention and treatment programs to meet the needs of those struggling with addiction and opioid use disorder. Exacerbating this challenge is the fact that MAT drugs and programs are not made available to all women equally-which particularly impacts low-income women and women of color.
Recent research indicates that White substance abusers are disproportionately benefiting from prescriptions for buprenorphine, a MAT drug that reduces cravings for opioids and helps prevent overdoses. A recent assessment of two national surveys of physician-reported prescriptions, containing information on 13.4 million medical encounters, found that the number of buprenorphine prescriptions rose dramatically from 2012 to 2015. There was, however, no corresponding increase in the number of prescriptions written for African Americans or other people of color. The research suggests that White substance abusers are the ones primarily getting these prescriptions.
Additionally, because only about 5% of physicians have the special training required to prescribe buprenorphine, providers can effectively set their own price for these prescriptions. Three-quarters of patients either paid cash (40%) or used private insurance (35%) for their buprenorphine prescription. Poverty and lack of private insurance make buprenorphine inaccessible to many low-income individuals and people of color. The result is that White Americans “are almost 35 times as likely to have a buprenorphine-related visit than Black Americans.”
To address these problems, regulators can eliminate requirements for special training in order to prescribe buprenorphine, set caps on the number of substance-abusing patients a provider can manage on the drug, and expand access to MAT throughout a broad array of primary care settings.
Even when treatment options appear to be accessible, there may be structural barriers that prevent women from being able to use them. A critical barrier is the lack of child care in substance use treatment centers, since approximately 70% of women entering these centers have children. Yet in 2017, only 6.4% of outpatient substance use treatment centers that serve women provided child care for their patients. Women getting treated at the other 93.6% of facilities face an added obstacle in finding and paying for child care, an impossible hurdle for many.
Providing free or low-cost child care for mothers in treatment would greatly reduce barriers to needed care. Family-centered treatment is designed to address this problem by providing services for both parents and children. With family-centered treatment, women can meet their parenting responsibilities, bond with their children, and access child care while fully participating in treatment. In addition, states and communities can support programs that focus on keeping mothers and children together. For example, the Family Group Decision Making programs seek to avoid the instability and trauma of separation by creating a concrete plan of action for the mother that includes interviews, a family assessment, and clear consequences in the case of relapse.
The NWHN has always advocated for women’s voices to be included in health programs, policymaking, and research design to ensure they collectively address our needs. The opioid epidemic is no different. Legislators, regulators, providers, insurers, and advocates must support evidence-based, multi-pronged approaches that recognize and address women’s unique experiences with opioid use disorder and opioid dependency.
We are starting to recognize what prevents and treats substance use and addiction: prioritizing women’s wellness over drugmakers’ profits; increasing access to the full range of health services; and incorporating evidence-based and thoughtful interventions over punitive ones. We need more research on women’s specific experiences with respect to addiction, however. We need stronger political, financial, and regulatory will to support programs and policies that actually work. Together, we must address the racism and systemic inequalities that disproportionately burden the marginalized and disenfranchised in our communities. Only when all these elements are in place will we turn the tide of this epidemic and be able to effectively address its devastating impact on women and their families.
Updated 2023


