

Your Health Unlocked Episodes
048: Living with PCOS and Hashimoto’s – Jaclyn’s Story
June 27, 2024
---

Campaigns
Publication Date: August 14, 2022
By: NWHN Staff

We are encouraged by the tremendous progress made in the last 40 years in LARCs design, safety, and efficacy. We strongly support the development of, and access to, the full range of safe and effective contraceptive options. And, we advocate for the elimination of financial, regulatory, and social barriers that prevent women from getting LARCs.
Yet, the NWHN is deeply concerned that enthusiasm for LARCs threatens individuals’ ability to decide which methods are best for their unique circumstances. Aggressive promotion of LARCs-or of any method-infringes on reproductive autonomy and can’t be separated from the broader context of reproductive coercion.
The Network is particularly troubled by reports-confirmed in a number of qualitative studies-that providers and public health officials are promoting the use of LARCs regardless of a person’s independent sexual and reproductive health needs, desires, or family planning priorities.
While we continue to fight rampant, on-going attacks on access to contraception and abortion care, we must also protect and defend reproductive autonomy from coercive programmatic and provider practices. Every person must have complete information about all of their contraceptive options and be able to choose the method that is right for them without any cost or access barriers.
It’s not possible to understand present-day LARCs coercion or its lasting impact on marginalized communities without understanding the broader context of reproductive coercion. From our nation’s founding, controlling Black women’s fertility was a cornerstone of slavery, while exterminating Native women and their children was an explicit part of our frontier policy. Beginning in the early 20th century, sterilization laws began formally targeting women of color, low-income women, immigrant women, and women with disabilities. In 1927, involuntary sterilization received the blessing of the US Supreme Court in the infamous Buck vs Bell decision. By 1965, one-third of all Puerto Rican mothers aged 20-49 were sterilized, many without their knowledge or consent. In fact, the procedure was so common on the island that it was simply called “la operacíon.” Because of the euphemism “tying the tubes,” many women didn’t realize that the procedure was permanent. Future Network board member Helen Rodriguez-Trias played a key role in bringing national attention to widespread sterilization abuse there. Meanwhile, throughout the 1960s and 70s-as documented by the award-winning film No Más Bebes-hundreds of immigrant women in California were pressured into signing sterilization consent forms mid-labor or under threat that their babies would die if they refused to sign.
By the 1970s, the newly-formed Network was testifying at nationwide hearings on proposed federal sterilization guidelines and recruiting volunteers to speak up in their communities about sterilization abuse. And while it’s tempting to think of state-sponsored sterilization abuse as ancient history, doctors in the California prison system were caught coercing female inmates into sterilization against their will as recently as 2010.
The parallels between sterilization coercion and LARCs coercion became clear within days of FDA approval in 1990 of the first LARC-the implant Norplant. Like involuntary sterilization, LARCs coercion immediately targeted women of color, low-income women, immigrant women, and women with disabilities. The Philadelphia Inquirer asked, “Poverty and Norplant-Can Contraception Reduce the Underclass?” while the Washington Post reported on a radio talk show host who proposed requiring all young girls reaching puberty to use Norplant. State legislators nationwide soon picked up the cause, pushing legislation to make Norplant mandatory for low-income women receiving public benefits or making it a part of court sentences.
In recent years, we have seen this same underlying principle play out in states like California, where, until 2016, women with more than two children were ineligible for additional public benefits unless they were using LARCs at the time they became pregnant. And we’ve seen it in states like South Dakota where, up until The Network began calling attention to it in 2017, the state Medicaid program explicitly refused to cover the removal of a LARC if the intent was to become pregnant.
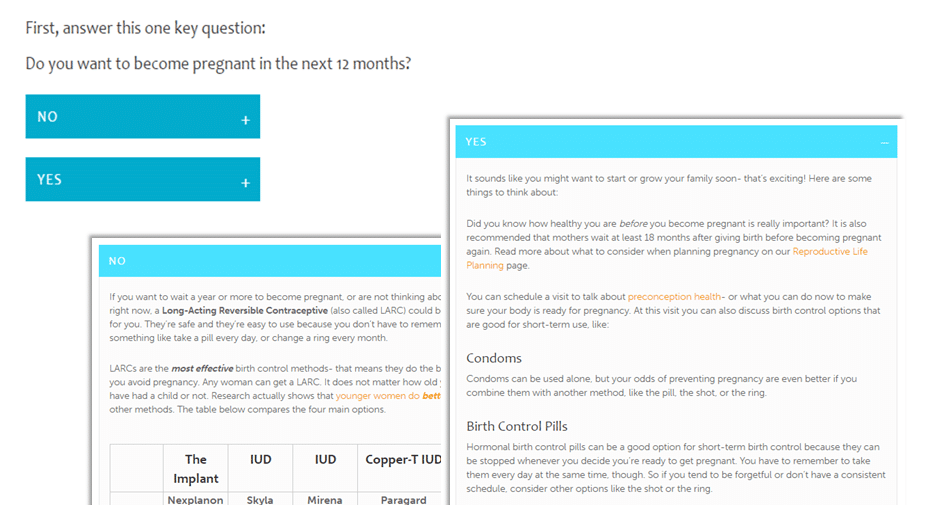
Meanwhile, more subtle forms of contraceptive coercion play out in clinics around the country when women are pushed to choose a LARCs method, no matter what their true reproductive priorities might be. Up until The Network called attention to it in 2016, for example, one state public health website strongly implied that there were right and wrong contraceptive choices. Site visitors hoping to learn more about their contraceptive options were directed to first answer the question, “Do you want to become pregnant in the next 12 months?” Respondents could click “No” for information about LARCs methods, but to learn about any other methods, they had to click “Yes,” suggesting that methods like the pill, patch, or ring would lead to pregnancy.
In partnership with the National Institute for Reproductive Health (NIRH), we developed a toolkit to help activists evaluate and shape LARC policymaking at the state level.

Watch our May 2019 webinar on the history of LARC coercion and how activists can use the toolkit to effect change in their states.
Watch Video
Statement of Principles
These examples and more are why The Network joined with our allies at SisterSong to craft a statement of principles to guide the non-coercive provision of LARCs:
“We believe that people can and do make good decisions about the risks and benefits of drugs and medical devices when they have good information and supportive health care. We strongly support the inclusion of long-acting reversible contraceptive methods (LARCs) as part of a well-balanced mix of options, including barrier methods, oral contraceptives, and other alternatives. We reject efforts to direct women toward any particular method and caution providers and public health officials against making assumptions based on race, ethnicity, age, ability, economic status, sexual orientation, or gender identity and expression.”
“We believe articulating these principles is necessary to protect the bodily autonomy and to respect the agency, health, and dignity of marginalized women so that those who have historically been oppressed or harmed feel safe when making reproductive decisions. This is a critical step forward. This is what reproductive justice looks like.”
Hundreds of national, state, and local organizations and individuals have endorsed the statement. This is a living document shared by Sister Song and The Network.


